As I have become increasingly frustrated with misinformation in the media, I found it necessary to put this guide together.
Here is some factual information about the virus, what kinds of masks you SHOULD and SHOULD NOT wear, and additional safety measures that you NEED to take when out in public.
Please share this with others, and stay safe.
Table of Contents
Size and Distribution of Virus Particles

On the right is a standard U.S. 25 cent quarter dollar coin, which should appear on your screen at about its actual size – about 1 inch.
In the middle, that quarter is enlarged 4x – it should be about 4 inches in diameter on your screen.
On the left is an enlarged sneeze droplet – in real life, the largest airborne sneeze droplet is about 1mm in diameter, but here it’s shown 4 times its size (about 4mm)

Above is a chart showing sneeze droplet distribution by size – the number of droplets you can expect to find based on its size, within a single sneeze.
As we move to the right, the droplet size increases. As we move to the left, droplet size decreases.
For a given size across the bottom, the higher the line is at that point, the more droplets of this size you can expect to find in a sneeze.
On the right is our 1 millimeter (mm) droplet – this is 1/25 of an inch, and is the largest common airborne droplet you can expect to find.
The smallest common droplet is about 25/1000 of one millimeter, or 25 microns (25 um).
Although these are the practical limits, sneeze droplets can be larger or smaller.
This graph is an interpretation based on the data from this study:
Characterizations of particle size distribution of the droplets exhaled by sneeze
Z. Y. Han, W. G. Weng and Q. Y. Huang
https://royalsocietypublishing.org/doi/full/10.1098/rsif.2013.0560
11/6/2013
The other finding in the study is that, in general, healthy people expectorate smaller particles, while in general, sick people expectorate larger particles.
As of this writing, we think one of the reasons COVID-19 is so infectious is that seemingly-healthy people can expectorate infected particles, which means that we can expect very tiny, infected particles.

In the above chart, we are showing the same information, but the scale is a logarithmic one.
As we move from the right, starting at 1mm, and moving left, each mark across the bottom is 10 times smaller.
- The first mark is 0.1 millimeters (one tenth) or 100 microns (um).
- The next mark is 1/10 of that – 10 microns.
- Next is the 1 micron mark. 1000 microns = 1mm
- To fully understand the size of COVID-19, we need to go in to the nanometer scale – the left edge is 100 nanometers, which is 0.1 microns.

On the above chart, we have some specific sizes marked – left (smallest) to right (largest):
- The COVID-19 virus is about 140 nanometers, which is 0.14 microns, which is 0.00014 millimeters
- The smallest possible infected sneeze droplet is about 200 nanometers (0.2 microns)
- There has been a lot of coverage about N95 masks – NIOSH N95, N100 and HEPA all filter particles 300 nanometers or larger. This is also the smallest particle able to be filtered by MERV 16.
- MERV 13 through 16 are all designed to filter particles 1 micron or larger.
- Surgical masks and inserts are rated at “PM 2.5” – they are designed to filter out particles 2.5 microns or larger.
- MERV 9 through MERV 12 are designed to filter particles in the 1 to 3 micron range or larger.
- A decent water filter traps particles 5 microns or larger
- MERV 5 through MERV 8 are designed to filter particles in the 3 to 10 micron range or larger.
- A good quality coffee filter can remove particles larger than 15 to 20 microns
- A crappy coffee filter can remove particles larger than 20 to 30 microns
- The oil filter on your car operates in the 40 micron range
- A 180 thread count cotton surgical mask with no insert operates in the 150 micron range
- The media has been stating that “at least a T shirt is better than nothing” – a typical cotton T shirt will only filter to about 500 microns – half of a millimeter. A cotton T shirt is about the same as nothing.

To understand the scale, let’s look at some nano-scale particles:
- A typical cold virus is in the 30 nanometer range. These are extremely simple and small.
- COVID-19 is a much larger Corona virus, which can range from 120 nanometers up to 300. COVID-19 is on the small side for a coronavirus, at 140 nanometers.
SARS and HIV are also members of the corona family. Due to their large size, the virus can’t survive long outside the human body without the shell breaking down. This is the reason that HIV isn’t airborne, and that you can’t catch it from a toilet seat. - The smallest possibly-infected sneeze droplet is about 200 nanometers – about 60 larger than the virus itself.
- The filtration limit of NIOSH, HEPA, and MERV filters is 300 nanometers – about twice as large as the bare virus, and 1/3 larger than the smallest sneeze particle.
Effectively, this means that the virus itself, as well as some very tiny virus-infected particles can pass right through even the best commercially-available filters.

Moving up the scale, we see that the 3 micron filtration limit of MERV 12 is huge compared to the virus, smaller sneeze particles, and even NIOSH / HEPA filter pores.
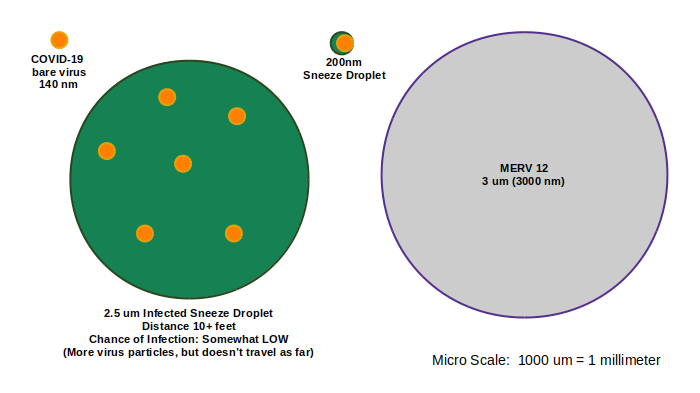
A 2.5 micron infected sneeze particle, containing multiple copies of the virus, could pass through a 3 micron MERV 12 filter.

As we continue to move up the scale, particles become larger. Although they could be more infectious because they *might* carry more copies of the virus, they don’t travel as far, and are easier to filter.
This is one of the reasons why social distancing is important – the farther you are from someone, the less likely you are to encounter larger, more infectious particles.
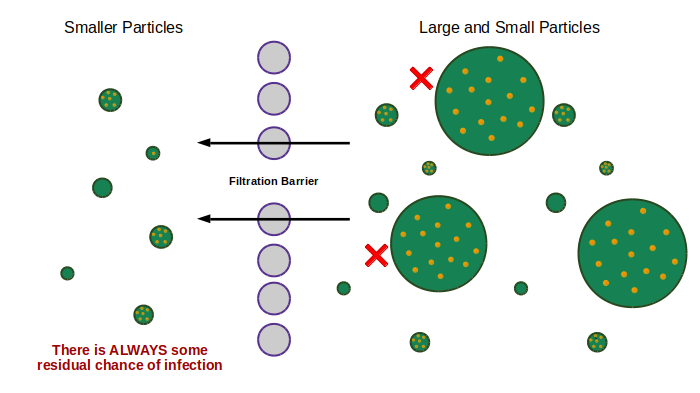
Regardless of what kind of filter you use, there is always some residual chance that some infected particles will get through.
The best plan is to use the best filter available, to ensure that any residual particles are as small as possible, and least-likely to infect you.
NIOSH (N95) – Decoded
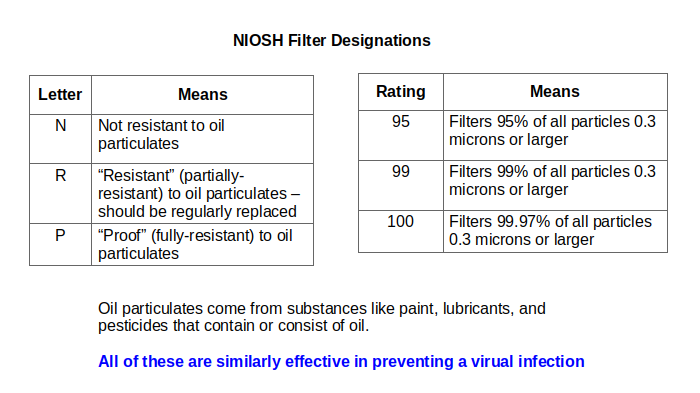
There has been a lot of media coverage about “N95” masks – N95 is part of the NIOSH rating system, and means that the mask in question will block 95% of particles 0.3 microns (300 nanometers) in size. Larger particles are blocked with greater efficiency.
“R” and “P” masks are the same as “N” masks, except that they don’t break down when exposed to oil particulates such as paint, pesticide, and vaporized lubricating oil.
N100 (or P100 or R100) is the equivalent to a HEPA filter, and is also the limit of a MERV 16 filter that you might use in your air conditioner.
All of these are just fine for preventing viral transmission.
Safety Gear – What you Need to Know

COVID-19 isn’t really airborne – it travels inside spit and snot particles that become airborne when an infected person sneezes or coughs.
Larger particles travel only a few feet, in a “ballistic” (arc) trajectory, while smaller particles form a mist that can carry 20 feet or more by floating in the air.
Larger, more infectious particles are more affected by gravity (thus the need for social distancing), but smaller particles can travel much further, and even though they are less infectious, your chances of becoming infected go up based on your level of exposure.
When an infected snot / spit particle comes in to contact with your mucous membranes in the mouth, nose, lungs, or eyes, the virus can pass through them, and you might become infected.
The more often this occurs, the more likely you are to become infected.
Also, some of those airborne particles are prone to land on flat surfaces, where they lay in wait for you to touch them. When this happens, they transfer to your hand, and when you then touch your eyes, mouth, or nose, you can become infected.
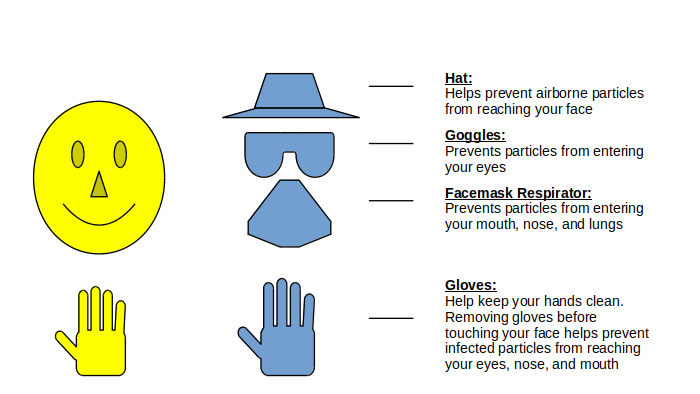
If you have enough reason to wear a mask in public, you should also wear goggles, gloves, and a hat.
If you ONLY wear a mask, your eyes are exposed. A mask can’t protect your eyes.
Wearing a hat and gloves helps keep infected particles away form your face.
Masks and Respirators

Although a full facemask respirator covers the entire face, and thus provides the best protection, these are expensive and somewhat impractical.
All the rest require some form of eye protection in order to be reasonably effective.

A full facemask respirator is basically the same as a half-mask respirator, except that it includes a face shield.
Both have removable cartridges that need to be periodically replaced – ideally, every time you go out in public, but this isn’t practical. Replacing them once a day is good, and every other day is adequate.
Likewise, the inside of the mask should be cleaned and disinfected daily – be sure to remove the cartridges BEFORE you clean the mask, and replace them afterwards.
Wearing any kind of respirator mask puts strain on the lungs, and should therefore be worn as briefly as possible.
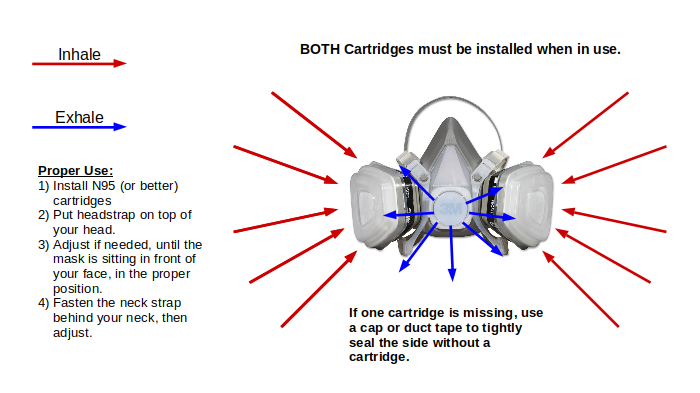
- When you use full or half mask respirator, air enters through slits in the cartridges. As you exhale, air leaves the mask through the valve in front.
- Be sure to use NIOSH N95 rated cartridges or better – any NIOSH rated cartridge will do.
- You should always use 2 cartridges, but if you only have one cartridge, be sure to cap off the other filter hole, or use duct tape to create an airtight seal. Using only one cartridge means that it must be replaced more frequently.
- Make sure the mask is worn properly – the straps should be tight, and there should be no gaps between the mask and face.

Disposable filters can be a cost-effective solution, but should be discarded after one use.

Some disposable respirators have an exhalation valve that keeps the mask cool and allows for easier breathing.
Leakage occurs when the mask isn’t properly fitted to the face, allowing unfiltered air around the edges.
- Always make sure the mask fits as tightly as possible
- Always check for gaps and adjust the nosepiece

Make sure you get NIOSH-rated masks. Plenty of companies sell “dust masks” that look just like a true respirator mask, but they are nothing more than a glorified coffee filter.

“Surgical masks” are the most comfortable, but offer the least protection.
Actually, the term “surgical mask” is a misnomer – they are called “earloop masks” or “procedure masks”, and they are designed primarily to protect other people from the wearer’s spit and snot. Actual surgeons wear NIOSH N100 disposable respirators.
The media says that you should at least wear a cloth mask because “that’s better than nothing”.
That’s like saying a holey umbrella is better than no umbrella. Wearing a cloth-only mask is exactly as helpful as wearing nothing, but gives the wearer a false sense of security. Cloth-only masks should not be used at all.
Instead, use a reusable filter mask with a coffee filter as the insert.

The disposable kind offer minimal protection, but look for PM 2.5 rated and FDA approved.
Make sure you get masks with a bendable nosepiece – a wire across the top that can be molded to the shape of the nose.
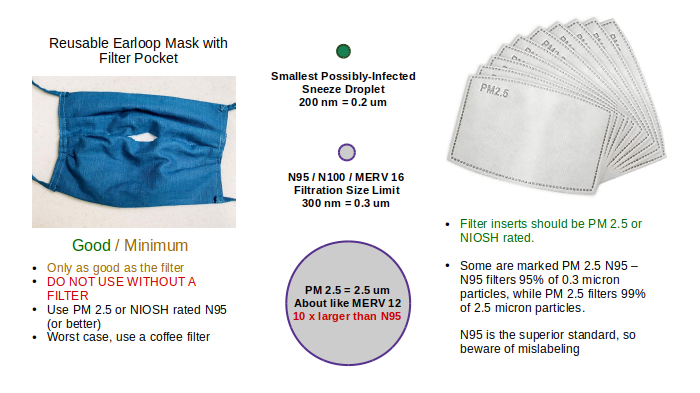
The reusable kind are far superior, because you can use any kind of filter, including N95. Filters should be changed after each use.
There seems to be a lot of confusion about the filter inserts – many are marked PM 2.5 N95. PM 2.5 is only guaranteed to filter down to 2.5 microns, but a true NIOSH N95 mask filters down to 0.3 microns – about a tenth of the size, and would include particles in the PM 2.5 range.
Buyer beware. Always look for ratings and certifications that you can look up or cross-check online – if a specific mask is FDA approved, it will be listed on their website.
If a filter is NIOSH rated, the manufacturer should be able to provide a certification to back up that claim.
Eye Protection

In order for your eyes to be protected from infection, you need to wear eye protection that keeps particles away from them – even small, airborne particles.
This is why you need goggles, not glasses.
Goggles form a seal against your face, completely covering your eyes. Glasses have large openings around the cheeks, temples, and nose that allow airborne particles in toward your eyes.
“Contour” glasses are not goggles, but they closely follow the contour of your face, preventing all but small particles from entering your eye.

None of these protect you.
All of them allow airborne particles to travel in to your eyes around the sides, top, and bottom.
“Vented” goggles are as good as NO goggles.
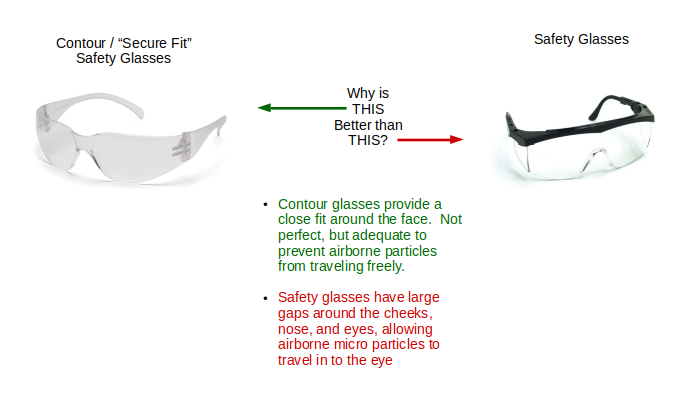
Unlike regular safety glasses, “contour” glasses can be fitted at least somewhat tightly against the face.
Why COVID-19 is Worse Than a Regular Flu
In order to explain this, I’m using made-up data, so don’t run off and think that these curves are accurate – they are a model that I can use to illustrate the problem, and there is no actual data behind them.

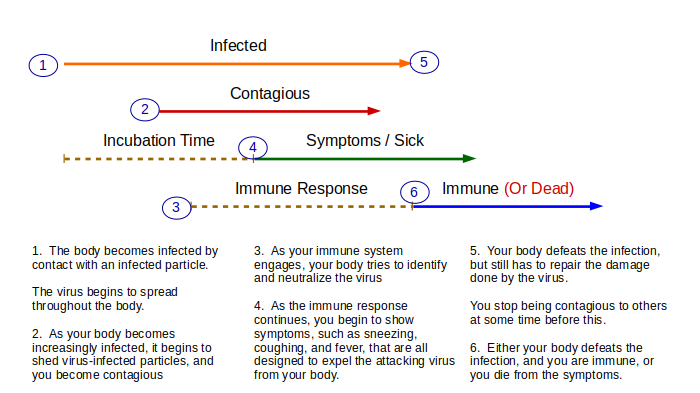
When you become infected by a normal virus (blue), the infection builds in your body until two things happen:
- You start to expectorate infected particles, and thus you, yourself become contagious to others
- Your body’s immune system begins to kick in, and you start to experience symptoms
With a normal flu, all of this happens within a few days of infection – you begin to show symptoms at around the same time you become contagious.
People see that you are contagious, and they know to stay the hell away from you.
Likewise, as you start to have symptoms, you are more likely to feel sick and stay home.

If we compare a “normal” flu to COVID-19 (again – NOT REAL DATA), there are 4 things that, in combination, make it very dangerous:
- Infected people appear to become contagious more quickly – perhaps even before they show any severe symptoms.
- Because the gap between being contagious and symptomatic, infected people can walk around in public, infecting others who are unaware because the infected person doesn’t have any severe symptoms.
- Once you become infected, COVID-19 appears to spread quickly inside the body. An infected person goes from infected and asymptomatic, to showing severe symptoms in a relatively short period of time. In the body’s weakened state, the immune system is compromised, and susceptible to other, secondary infections.
- COVID-19 brings severe respiratory symptoms with it – victims basically die of pneumonia.
As of this writing, there is about a 3% mortality rate. That means that if you put 33 infected people in a room, one of them is likely to die.
As of this writing, about 5,000 US deaths, January to present, have been confirmed to be a result of or involved COVID-19
The So-Called Question of Immunity
I keep hearing the media say “we’re not sure if a person can get reinfected or not”
Other than highly-specialized antiviral drugs, there is no way to “cure” a viral infection. Antibiotics help boost the immune system, and help prevent secondary infections (such as pneumonia), but they don’t kill the virus.
The only thing that can kill the virus is your body’s immune system.
Therefore, one of two things can happen, once you become infected:
- You stay infected until you die
- Your body beats the infection and you become immune
Let me qualify both of those statements:
- You stay infected until you die – HOWEVER, there are viruses such as HEP-C that allow the host to live for a very long time, but until recently, there was no “cure” for HEP-C – if you got it, you died with it. Likewise with HIV. Unfortunately, COVID-19 is not one of those.
- Your body beats the infection and you become immune – UNTIL the virus mutates, OR you lose immunity over time.
So when the news says “we’re not sure if a person can get re-infected” there is only one answer: NO YOU CAN’T (however, you might get infected by a mutated version of the virus, or you might lose your immunity years later and become reinfected at some point in the future)
BUT YOU WILL NOT GET REINFECTED TOMORROW. Nor next week.
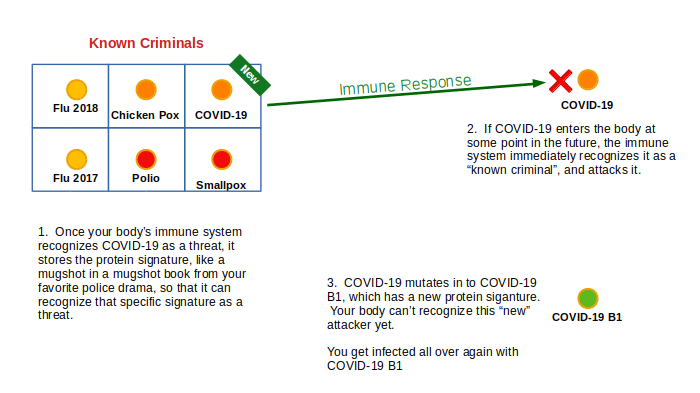
When your body’s immune system responds to a virus, it keeps a record of its protein signature – sort of like the books of mugshots that you see in police TV dramas.
When your body sees a protein that it recognizes, it immediately attacks and kills it.
Once your body knows that COVID-19 is a threat, your body begins to kill the virus.
However, if the virus mutates, it has no idea that the new version is also a threat.
Vaccines

The way a vaccine works, is that it introduces your body to the protein signature of a dead virus without the harmful payload. If enough virus particles enter the body, it adds the virus to its mugshot book, allowing your body to instantly and immediately repel the “real” virus later.
The problem with a vaccine is that the “version 1” vaccine doesn’t include any future mutations.

Once the virus mutates (they all eventually do), there needs to be an updated version of the vaccine that includes both versions.
Other Preventative Tips
- Avoid eating out at all. Even though many restaurants offer drive-through, carry-out or delivery service, all it takes is one careless sneeze for you or a loved one to become infected.
If you do eat out, check your city’s health department to make sure you only eat food from restaurants that got an “A” rating on their last health inspection.
Likewise, call the restaurant and ask the manager what special cross-infection precautions are being taken to prevent YOU from getting infected by THEM, THEM from getting infected by YOU, and YOU from getting infected by OTHER customers. If the manager can’t answer those questions adequately, don’t eat there. - Start getting in the habit of wiping off the mail and groceries and anything you buy before you bring it in to your house, and then start wiping things off again before you use them.
When you order something online, start getting in the habit of putting on gloves before you open it, and wipe off your items as you unpack them. - Social distancing applies when you’re in the car, also. We tend to think of our car as a bubble, but it’s not. Try not to park or stop right next to another car, especially if they have the window down. Make a habit of driving with your windows up.
- There is no half-measure. Either you’re concerned enough to wear a mask, glasses, gloves, and a hat, or you’re not. Don’t wear just a mask.
- DO NOT sign up for the “version 1” vaccine, unless you are at extreme risk. It will be risky for you, and problematic. It won’t contain any inevitable mutation, meaning, you will have to get re-inoculated later.
- For a decent disinfectant, add about 2 ounces of chlorine bleach to about 1 gallon of water. In a pinch, this can be used externally for hands, etc, although the chlorine might cause some irritation. Also, chlorine starts to break down when exposed to air and light, so only mix what you need to use right now – it can’t be stored.